Pfizer and AstraZeneca Covid-19 Vaccines now in stock. Click here to claim yours today!

Hello, Dr Matt from The Barracks here again. Today I get to talk about one my passions in medicine – skin cancer. I have always had an appreciation of the importance of skin cancer even during my training as a GP in England. The reason I enjoy skin cancer medicine is that it is one of the few cancers that can be picked up early relatively easily – you can literally see it – and also, if caught early, the cure rate is exceedingly good. Catching it early is the key, however, like any cancer. I’m going to divide this presentation into discussing the 3 common types of skin cancer, other benign skin lumps and bumps that can cause anxiety or look unpleasant and finally what we can all do to prevent harm from skin cancer which centres around prevention and early detection.
I’ve completed lots of post graduate education including certificates in Skin Cancer Medicine and Dermatoscopy, I’m about to complete my Diploma in Skin Cancer Surgery, I’m still studying a Masters in Skin Cancer through UQ. In addition, I’ve just signed up for an Aesthetic Medicine course which will allow me to perform Botox and Fillers (so watch this space!) During my time in Cairns, I worked as a GP with Special Interest in Dermatology in the public hospital alongside the specialist Dermatologist as well as assisting another specialist colleague set up his Mohs Surgery service.
In short, since moving to Australia, I have studied lots about skin cancer, I’ve seen lots of it and treated lots of it.
The word cancer causes anxiety in many people since it conjures images of very unwell and underweight people receiving chemotherapy and sometimes eventually losing their battle. Advanced cancer of any type is serious, and no cancer should ever be ignored or taken lightly, but not all cancers behave in the same manner. For instance, many skin cancers, if caught early can be completely treated relatively easily.
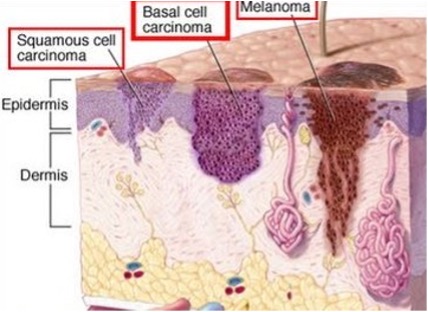
Within skin cancer are 3 most common types; these are called Basal Cell Carcinoma (BCC), Squamous Cell Carcinoma (SCC) and malignant melanoma. Of the three of these, melanoma is the most serious as it has the greatest risk of harm to people. This is because it can invade locally and spread to other sites early and pose greatest risk to life, whereas SCC tends to spread later and BCCs almost never. For this reason, we often bundle BCCs and SCCs together as “non-melanoma skin cancer”.
BCCs and SCCs arise from cells present in the top layer of the skin, called the epidermis. BCCs arising from the basal layer which separates epidermis from dermis. Melanoma arises from cells which produce pigment in the skin which can be present in the lower epidermis or the dermis, which is the layer below the epidermis.
BCCs and SCCs present either with a scaly lump that may grow steadily and itch or feel painful, or an ulcer which won’t heal or a smooth lump that may or may not be pigmented. BCCs and SCCs most commonly occur in sun exposed sites of the body meaning ears, face, neck, chest, shoulders, back and legs. They are usually related to sun exposure and more common in light coloured skin.

Typically, melanoma presents as a dark, flat mole which looks odd, asymmetrical and changes rapidly. However, melanoma can also change slowly or present as a lump or nodule and confusingly, some melanomas don’t even produce pigment and can be flesh coloured. Although some melanomas do arise in sun exposed sites and are similarly associated with sun exposure and light skin, some can appear literally anywhere on the body including where the sun does not shine and can occur in any skin type.

Recognising the different types of skin cancer can be a challenge and requires lots of training and experience for clinicians, but to keep it simple my advice to patients is to report any new, or changing moles, new lumps or sores which aren’t healing – the key here is new or changing. If you’ve had a dark mole for the last 20 years and it hasn’t changed, then most likely it is absolutely fine, but if you suddenly discover a new mole, or an old one changes, then this should certainly be shown to a doctor – either your family GP, a GP with interest in skin cancer medicine or a dermatologist.
A simple acronym to remmeber the things to look out for in melanoma is the ABCDE rule which reminds us to look for
A = Asymmetry. A chaotic lesion that is different on one part to another
B = Borders. irregular bordered lesion which is has blurry or jagged edges
C = Colour. A lesion with more than 1 colour
D = Diameter. A lesion greater than 6mm is usually more suspicious (but melanomas start smaller but are harder to identify when small)
E = Evolving – change. Cancers don’t stay static and will always change, though sometimes slowly.
The melanoma above shows a lesion showing ABCD and we can imagine E as well.
A skin cancer doctor will take a full skin history which includes asking about any skin lesions of concern but also previous skin problems including cancers, estimating past sun exposure, assessing a patient’s skin type which predicts risk of skin cancer, family history of skin cancer and other past medical problems.
They will then perform a complete skin examination which means inspected almost every part of the body – the genital areas aren’t routinely examined unless a problems is reported there, but it is still important that you inspect yourself every so often, using a mirror or a partner to look. If there is any doubt then of course a doctor will inspect for your, and for ladies this is most easily done during cervical screening.

They will then assess a new lesion or one of concern carefully both with the naked eye and then use a device called a dermatoscope which provides a magnified and bright image of the skin, usually using polarised light or some transparent gel to reduce light scatter from the surface of the lesion to allow better view of the upper layer of the skin. Dermatoscopy has come a long way in the last 30 years and now there is very good evidence that, with correct training, a skilled doctor with a dermatocope can distinguish cancerous from non-cancerous lesions in many cases. This allows for very early detection of skin cancers and reassurance where things are benign. Where there is doubt, it allows us to decide which lesions do need further assessment and this is usually with a biopsy.
A biopsy means removing a sample of the lesion, or sometimes all of the lesion, in a small surgical procedure under local anaesthetic. This is then sent to a lab where a trained specialist doctor, called a histopathologist, will look at slices of the lesion under a microscope and after applying special dyes can usually confidently confirm where the lesion is a cancer or not. This allows us to definitively reassure people where a lesion is benign, or where it is a cancer, guide further treatment if it wasn’t already adequately completely removed in the biopsy.
In some cases, for example superficial SCC or superficial BCC, treatment can be then completed using topical cancer creams, cryotherapy with liquid nitrogen or other less cosmetically damaging treatments.
In malignant melanoma, however, even if the lesion was removed completely the first time, going back to take a larger amount of surrounding tissue to reduce the chance of recurrence. This is because if melanoma does spread to other sites it has the highest risk to patients.
There are many things which appear on our skin which are benign – not cancers – but can still cause concern to patients. One of the challenges in clinical medicine for all doctors is recognising normal from abnormal and dermatology is no less a challenge. When doctors are conducting a skin check we can normally very easily, quickly and accurately categorise what is normal and abnormal and apparently pass over things which may cause you worry. If that is the case, and you were worried about something, please ask us so that we can explain and reassure you.
The medical word for mole is a Naevus and there are many different types of naevi. Some are present from birth (or appear within the first 6-12 months of birth) and are called congenital naevi. Others occur later in childhood or early adulthood and are called acquired naevi. Generally, congenital naevi produce lumps and may or may not be pigmented. Acquired naevi generally are flush with the skin and are usually pigmented. There are many different types of course and again recognising and naming them all can be a challenge, but the thing to remember as a patient is to report new or changing moles, particularly if they appear chaotic or asymmetrical. Benign moles will grow and change slightly in adolescence and may be benign, but if any mole is changing quickly or there is any concern, then go to see you doctor. It is also rare for a new mole to appear after the age of 25 and this would be considered suspicious in itself if one did.
Although some moles can become cancer (change to melanoma) most moles do not and in fact most melanomas (90%) do not arise in pre-existing moles. This is why a skin check that only looks at known moles can miss some cancers. Having many moles on your body (>200) is a risk factor for developing melanoma but again, most melanomas won’t develop in a pre-existing mole but having many moles tells us something about the genetic risk of that patient.
One the common skin lesions that appear in many people as we get older are Seborrheic keratoses, or “Seb Ks”. These are related to skin type, genetics and also sun exposure and they occur most commonly on the trunk, back and face. They may start as a flat, flesh coloured or light brown oval and symmetrical lesion but over time can become raised and more darkly pigmented – even deeply black. Despite this, we know that these are completely benign and don’t change into cancers. Although relatively easy for doctors to diagnose, they can certainly look a little odd and so as every if you have a new or changing skin spot or your have any concern, we will gladly have a look. Although they don’t become cancerous themselves, I have detected BCCs growing very close to a seb K. This is rare, but during a skin check I detected an odd, asymmetrical lesion which led me to cutting it out and so the cancer was still detected and cured. This highlights the need for skin checks (see below)

These are small, flat, pink, scaly sometimes itchy areas found in sun exposed sites. They occur owing to UV sunlight damage to the upper layer of the skin, the epidermis, and usually the squamous cells. They are considered pre-malignant for SCC meaning that they have the chance to become invasive SCC later. Most AKs won’t change but some can. If you have lots of these skin lesions then some treatment is advised, both for improved cosmetic appearance but also to reduce the risk of developing an SCC. Treatment can include freezing off visible lesions with liquid nitrogen (cryotherapy) or field therapy with anti-cancer creams. If a lesion is raised, or ulcerated, then it is unlikely to be a simple AK and may be an invasive cancer. In this case treating with freezing or creams is not appropriate and instead a biopsy ought to be arranged looking for cancer.

The best treatment is prevention in the first place.
There are risk factors for developing skin cancer; some of which we can change and some we can’t. Non-modifiable risk factors include; Previous skin cancer, a strong family history, our skin type, having red hair, having more than 200 moles and past sun exposure particularly burning regularly as a child. Ff you have any of these then you ought to consider having regular full skin examinations, at least annually, but for some people with previous skin cancers maybe more regularly.
What we can change is future sun exposure, in particularly preventing sun burn by avoiding the strongest sun in the middle of the day, covering up with clothing, sunglasses, wide brimmed hats and using-high factor sunscreen. These methods have shown a reduction in all skin cancers but particularly BCCs and SCCs. Other things we can do to reduce risk of skin cancer is to not smoke.
Prevention of serious harm from skin cancer can be achieved by early detection.
This is done both by people inspecting their own skin regularly, and getting partners, friends or family to help as well, and also by regularly skin checks by a doctor trained in skin cancer detection.
(Remember screening means looking for disease which may not be apparent. If you already have a suspicious skin lesion, then see a doctor and point it out to them).
Although anyone can have a skin check and all are welcome, if we are to have the biggest impact on health then targeting high risk individuals will have the biggest benefit. We’ve already discussed the risk factors and so we can predict the people at highest risk.
In descending order or importance
Thankfully, skin cancer in children is rare, but it can occur. Guidelines don’t advise that we routinely do skin checks in kids unless there are specific reasons to do so. If children have many moles on their body, or they are born with a large mole called a “giant congenital naevus” then regular checks may be needed. As ever, if there is any doubt, I recommend that you chat to your family doctor or your child’s paediatrician.
Skin cancer is common, especially in Australia and more likely in lighter skinned people, people that have had previous skin cancers and those that have burned a lot in their life. Most skin cancers can be treated effectively if caught early but melanoma, if not caught early, can kill. Checking your skin yourself AND getting a full skin check by a trained doctor is an important step in early detection, but sun avoidance and avoiding burning is the best way to prevent skin cancer.
If you ever see a new, or changing mole, spot, sore, lump then get it checked out straight away with your doctor. I always tell my patients that I’d rather see a hundred benign spots and reassure those patients than miss one melanoma that may end a life.